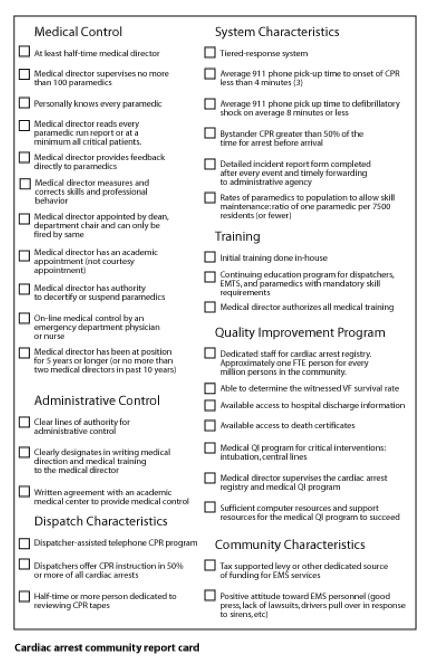
Cardiac arrest community report card
The report card shown is admittedly not based on science. There are no studies ranking community scores with survival rates though such an undertaking might be worthwhile. I would be the first to admit this report card contain subjective criteria. But I think the criteria are based in common sense and tinctured with science (for example, the relationships of intervention times and survival are clearly founded in science). The report card tries to be as specific as possible. Being too general allows every community to score high. Everyone probably has some form of quality improvement program but how many systems have a full time (or even part-time) person dedicated solely to maintain the cardiac arrest registry. Also it should be obvious that some of the elements overlap. For example, high bystander CPR rates correlate with lower average time from collapse to CPR. Given these qualifiers the following elements comprise the report card.
The cardiac arrest community report card is grouped into 7 categories: medical control, administrative control, dispatch characteristics, system characteristics, training, quality improvement program, and community characteristics. Medical control has the most elements. The medical director is ultimately responsible for the professional behavior of the paramedics. He or she should read every incident report and immediately address problems that are identified. They may be as mundane as legible writing (or complete data entry) or complete documentation. The problems may involve dealing with skill performance or medical decision making. (For example, the medical director may inquire why a 52 year old man with intermittent left sided jaw pain - a possible symptom of angina - was left at home.).
Raising your score
The scorecard has 35 elements - 3 points for each with a perfect score being 105. Though it might be enlightening to grade your community the real purpose of the scorecard is to suggest a way toward improvement. For every element that does not exist in your community ask if it should be and how it can be achieved. Parts of the scorecard are easy to improve and others present considerable challenges. It is not realistic to go from a failing grade to honors overnight. Change, as difficult as it may be, should be viewed as a continuous process. Though lack of resources, cultural impediments to change, inertia and complacency can be strong inhibitors of change the process must be undertaken. Those in EMS are health professionals. Thus they have a duty to their patients. This duty is uncompromising - to do everything possible on behalf of the patient. An EMT or paramedic is an extension of the medical director for that community. A physician encountering a patient, whether in pain, anxious, or unconscious in cardiac arrest, must do everything possible to help that patient. That is the obligation of every physician. And that is the obligation of every EMT and paramedic. And if the system is failing then we are failing our patients.